Vu Orthodontics - Orthodontics, Periodontics, and Implants
16027 Brookhurst St., Ste. K
Fountain Valley, CA 92708
ph: 714-775-0100
fax: 714-463-2205
drhungvu
Ortho, Perio & Implants
Root Conditioning
The root of the tooth must be conditioned mechanically and chemically prior to certain grafting procedures. The process of cleaning the root mechanically will inevitably create a smear layer which must then be removed. The best way to remove this smear layer chemically is by using ethylenediaminetetraacetic acid (EDTA) which is an amino polycarboxylic acid, a chelating agent, and a colourless, water-soluble solid.
Traditionally, dentists and endodontists use EDTA solutions to remove the smear layer and lubricate the root canals in endodontics. The EDTA solution for this application is in a liquid form.
RC-Prep is routinely used for the chemo-mechanical preparation of root canals. Contents: 10 % urea-peroxide, urea peroxide and 15% EDTA in a paste form (special water-soluble base).
EDTA in a gel form is commercially available as PrefGel, a pH neutral, 24% EDTA, a product of Straumann. It is a root surface conditioner, for topical application onto exposed root surfaces.
Citric acid: Its use for root conditioning must be avoided because it is acidic and it may cause root resorption. Its pH is typically reported as 2.2, but this value varies depending on the concentration.
Sutures
Many types of sutures are used in surgical dentistry. Each type has pros and cons, and different dentists have different preferences. Sutures classified as monofilament or multifilament (braided) and absorbable or non-absorbable.
Some clinicians prefer smooth monofilament sutures for better healing (mainly by avoiding "wicking" effect of braided sutures).
The wicking of the multifilament sutures at the surgical sites often causes prolonged inflammatory reactions. Monofilament sutures are advantageous in preventing bacterial wicking into surgical sites.
The most common sutures are
- Plain gut: monofilament, absorbable, will last about 1 day in the oral environment
- Chromic gut: monofilament, absorbable, will last about 2 weeks in the oral environment
- Silk: multifilament, nonabsorbable, must be removed no more than about 10 days
More advanced sutures are
- PGCL (Poly Glycolide Co-Caprolactone): absorbable, synthetic. The thread is smooth and soft. Note that PGCL suture is similar to Monocryl® suture.
Thread type: Monofilament
Color: Violet/ Undyed
Strength duration: 14-21 days
Absorb duration: 90-120 days (Source: AD Surgical). But, in the experience of the author, some knots are generally broken in about 1 month.
- Polypropylene: monofilament, nonabsorbable, synthetic. It is indicated for soft tissue approximation and ligation. Its advantages include minimal tissue reactivity and durability. Disadvantages include fragility, high plasticity, and high expense. Prolene® is the most popular polypropylene suture. Note that nylon sutures are less expensive and are similar to polypropylene. But some clinicians report that Prolene is relatively more innert and less cutting soft tissue than nylon. But according to Wikipedia, "Prolene is a synthetic, monofilament, nonabsorbable polypropylene suture. It is indicated for skin closure and general soft tissue approximation and ligation. Its advantages include minimal tissue reactivity and durability. Disadvantages include fragility, high plasticity, high expense, and difficulty of use compared to standard nylon sutures."
- Polyglycolic acid (PGA): multifilament (braided) absorbable, synthetic, dyed and undyed. The thread is soft, and knot secured. Note that PGA suture is similar to Vicryl® suture.
- Polytetrafluoroethylene (PTFE) -- also known as Teflon®: nonabsorbable. Unlike most monofilament sutures, PTFE is soft. PTFE sutures may be considered as quasi-monofilament, so they prevent bacterial wicking, somewhat. But unlike PGCL or Prolene, PTFE sutures must not remain for long (at the surgical sites). Note that because of the streching characteristis, PTFE sutures lose their strength, so they are not as good as they were thought to be. There are three (3) different types of PTFE sutures:
1. e-PTFE (expanded PTFE): GORE-TEX suture which is porous but it is easier to handle (better knot stability)
2. d-PTFE (dense PTFE): Cytoplast suture is relatively stiff so it is more difficult to handle (better knot stability) but less porous than GORE-TEX
3. PTFE: Omnia PTFE suture -- According to the manufacturer, the suture is less porous than GORE-TEX and less stiff than Cytoplast.
Suture Needles
Two (2) important types of suture needles are discussed here: "conventional" cutting needle (Fig. 1) and "reverse" cutting needle (Fig. 2)
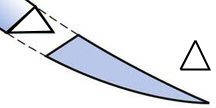
Fig. 1. Conventional Cutting Needle
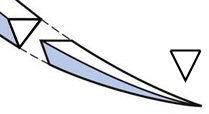
Fig. 2. Reverse Cutting Needle
“Conventional” cutting needles have the cutting edge on the concave surface (inner) and are useful for tough tissue, e.g., keratinized mucosa (masticatory mucosa which is keratinized stratified squamous epithelium).
On the other hand, “reverse” cutting needles have their cutting surfaces on the convex surface (outer) and are ideal for both tough tissue (e.g., keratinized mucosa) as well as delicate tissue (e.g., lining mucosa which is nonkeratinized stratified squamous epithelium).
Unlike conventional cutting needles, reverse cutting needles offer a reduced risk of cutting through tissue.
References
1. Michael S. Baggish, Suture Material, Suturing Techniques, and Knot Tying, Ch. 4
2. Oral Mucosa, Wikipedia
3. Szczepan Baran, Elizabeth Johnson, and Marcel Perret-Gentil, Understanding and Selecting Surgical Suture and Needle
4. Wayne W. LaMorte, Suturing Basics, Basics of Wound Closure and Healing
16027 Brookhurst St., Ste. K
Fountain Valley, CA 92708
ph: 714-775-0100
fax: 714-463-2205
drhungvu